116314
论文已发表
注册即可获取德孚的最新动态
IF 收录期刊
- 3.6 Breast Cancer (Dove Med Press)
- 4.3 Clin Epidemiol
- 2.6 Cancer Manag Res
- 3.2 Infect Drug Resist
- 4.1 Clin Interv Aging
- 6.1 Drug Des Dev Ther
- 4.1 Int J Chronic Obstr
- 8.7 Int J Nanomed
- 2.5 Int J Women's Health
- 3.2 Neuropsych Dis Treat
- 2.4 OncoTargets Ther
- 2.6 Patient Prefer Adher
- 2.6 Ther Clin Risk Manag
- 3.1 J Pain Res
- 3.5 Diabet Metab Synd Ob
- 4.5 Psychol Res Behav Ma
- 3.4 Nat Sci Sleep
- 2.4 Pharmgenomics Pers Med
- 2.6 Risk Manag Healthc Policy
- 4.6 J Inflamm Res
- 2.3 Int J Gen Med
- 3.9 J Hepatocell Carcinoma
- 3.3 J Asthma Allergy
- 2.5 Clin Cosmet Investig Dermatol
- 3.0 J Multidiscip Healthc

对老年房颤患者的两个年龄组进行临床特征和结果的比较
Authors Shao XH, Yang YM, Zhu J, Zhang H, Liu Y, Gao X, Yu LT, Liu LS, Zhao L, Yu PF, Zhang H, He Q, Gu XD
Published Date August 2014 Volume 2014:9 Pages 1335—1342
DOI http://dx.doi.org/10.2147/CIA.S67123
Received 2 May 2014, Accepted 27 June 2014, Published 12 August 2014
Background: Atrial fibrillation (AF) disproportionately affects older adults. However, direct comparison of clinical features, medical therapy, and outcomes in AF patients aged 65–74 and ≥75 years is rare. The objective of the present study was to evaluate the differences in clinical characteristics and prognosis in these two age-groups of geriatric patients with AF.
Materials and methods: A total of 1,336 individuals aged ≥65 years from a Chinese AF registry were assessed in the present study: 570 were in the 65- to 74-year group, and 766 were in the ≥75-year group. Multivariable Cox hazards regression was performed to analyze the major adverse cardiac events (MACEs) between groups.
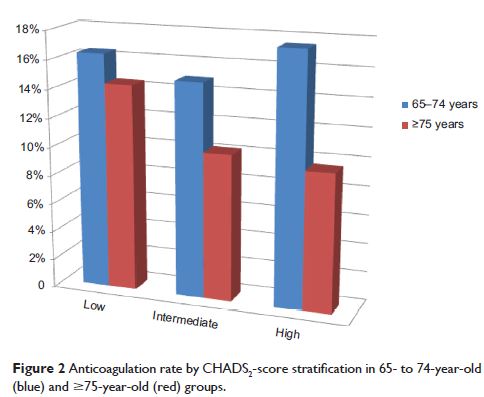
Results: In our population, the older group were more likely to have coronary artery disease, hypertension, previous stroke, cognitive disorder, or chronic obstructive pulmonary disease, and the 65- to 74-year group were more likely to have valvular heart disease, left ventricular systolic dysfunction, or sleep apnea. The older patients had 1.2-fold higher mean CHADS2 (congestive heart failure, hypertension, age ≥75 years, diabetes, stroke) scores, but less probability of being prescribed drugs. Compared with those aged 65–74 years, the older group had a higher risk of death (hazard ratio 2.881, 95% confidence interval 1.981–4.189; P <0.001) or MACE (hazard ratio 2.202, 95% confidence interval 1.646–2.945; P <0.001) at the 1-year follow-up. In multivariable Cox analyses, secondary AF diagnosis, a history of chronic obstructive pulmonary disease, and left ventricular systolic dysfunction were independent predictors of MACE in the older group.
Conclusion: Patients aged ≥75 years had a worse prognosis than those aged 65–74 years, and were associated with a higher risk of both death and MACE.
Keywords: atrial fibrillation, geriatric patients, mortality, major adverse cardiac events (MACE)